Sydenham Family Dental | Biological & Comprehensive Dentistry

YOUR BEST DENTAL EXPERIENCE
Neuromuscular Dentistry
'TMJ', Head, Neck & Facial Pain Disorders
What does this term mean? There have been many terms used over the years that basically are trying to capture the essence of dysfunction of the jaw joints ( there are two) and muscles of the head and neck (which are paired). When this system is out of balance, it creates dysfunction, pain, crooked teeth, head, neck and facial pain disorders,’TMJ’ disorders, impaired athletic performance and sleep disorders. At a very basic level, the cause for much of this is the same. Imbalance in the system. It was once explained to me, by an osteopathic physician, I believe, that the head is a highly specialized vertebrae. All vertebrae in our spine have three points of contact, like a three legged chair.
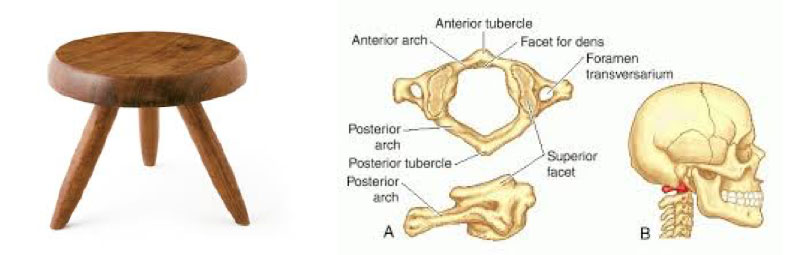
The exception is the head. It sits on two rockers (superior facets) with the vertebrae below (atlas). What is the third point of contact? The teeth!! Any impairment in how the teeth contact will torque and distort the connections and, more importantly, the paired muscles all the way down the spine.
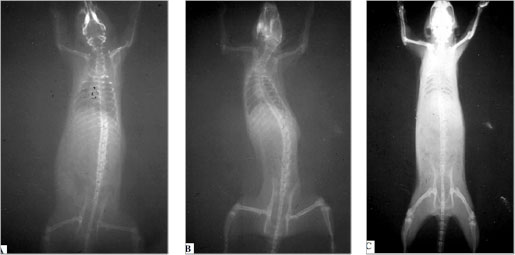
This was nicely demonstrated in rats by D’Attilio et. al. in the Journal of Craniomandibular Practice, April 2005. A plastic filling placed on the molar of a rat created a distortion in the bite called a scoliosis. It was corrected by the removal of the filling.
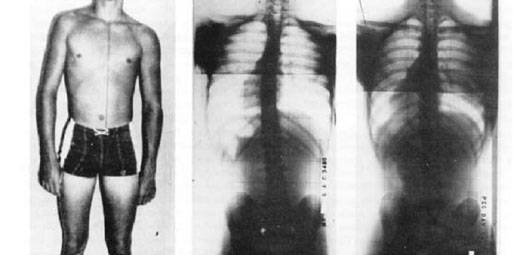
It was also demonstrated in humans by Dr. Al Fonder in his classic text ‘The Dental Physician’
(published in 1984), in this case using mercury fillings to ’balance;’ the bite.
But why does jaw torque cause problems? What is torque? The best analogy I can think of is the
position of a plane in the air. The positioning is described as having Pitch, Roll and Yaw.
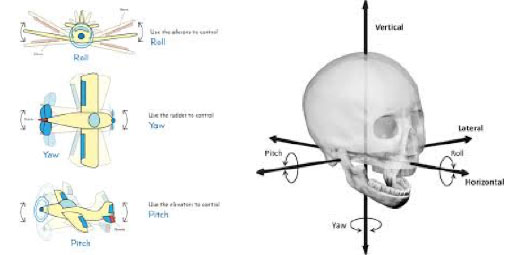
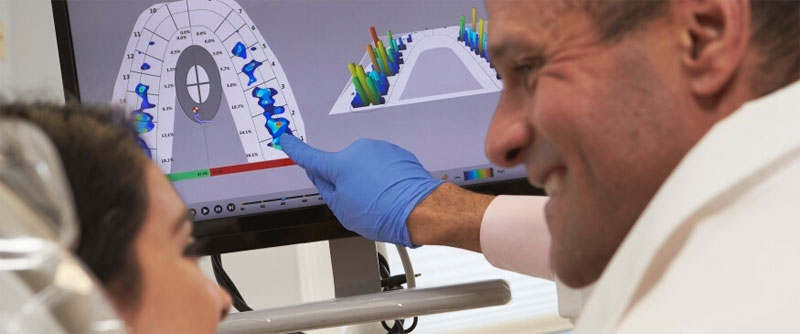
The same analogy can be used to describe the position of the lower jaw in space. As the lower jaw comes up to meet the upper teeth, in an ideal position, the paired muscles work evenly and when the teeth contact they are identical in the amount of force they put on the teeth. Sadly, most dysfunction, and pain and most of the other disorders are caused by uneven muscles, which sets up pain patterns in the unbalanced muscles. You see most people have two positions for their jaws. One where the teeth meet and all connect and another where the muscles are balanced and the teeth do not connect. The discrepancy between these two positions and the ability of the patient to adapt determines the pathology we see and feel. Pathology can mean many things but for us we see mainly tooth wear and breakdown and muscle fatigue and pain. Most therapy is geared toward alleviating symptoms rather than addressing the cause. The goal of any therapies working with ALL of these disorders should be to get the jaw in a position now referred as physiologic rest position (PRP). This position takes the torque out of the system and allows the muscles to heal. There are two problems with traditional therapeutic treatments: The first, using ‘splints’ or ‘nightguards’ or anything else put in the mouth, even dentures and sleep appliances are not made to the PRP, so although they have been reasonably successful, they still leave torque in the system and indeed can make things worse (like sleep apnea). The key being for the ‘successful’ cases is that the therapies have not exceeded the adaptive capacity of the patient. For most that cannot tolerate anything put in their mouths, often the reason is that the appliance or device has exceeded their adaptive capacity (there are many reasons). Most therapies are best practices taught over the years that seem to come close but at best are best guesses to the PRP. The ideal way to get to PRP is to be able to measure it objectively and there are instruments we use to do that. The primary instrument we use to objectively determine where to establish proper jaw position is the K7 computer evaluation system.

Once we have established the correct position, we verify it with a device called the TekScan , often referred to as the GPS system for the bite. This determines if the teeth are contacting correctly.
As Dr. Bob Jankelson used to say “If you can measure it, it is a fact, if you cannot, it is an opinion”. Much of my training over the last 25 years has been chasing the elusive PRP in patients who have very little adaptive capacity – the cases where the traditional therapies do not work. This whole area is fascinating and constantly evolving. For more in depth information, I urge you to explore the information in the links below.
For specifics on ‘TMJ’ and head neck and facial pain therapies these two sites are the most comprehensive: occlusiontmjauthority.com | www.leadingdentist.com
Snoring / Sleep Apnea Management
The standard of care for the treatment of sleep apnea is the CPAP device.
However, oral appliances are becoming more effective due to the fact that many of the same principles above are used to find the correct jaw position (PRP) to fabricate oral devices for snoring and sleep apnea disorders. We work in conjunction with sleep physicians who diagnose and prescribe sleep appliances for our patients. This is becoming the standard of care and no sleep appliance should be placed other than by a specially trained dentist. The key with these devices is that the position of the jaw must be in a position that does not stretch or create tension in the muscles of the jaw, neck and throat. Often these devices fail due to tension in muscles that can compromise the airway and make the condition worse, thus the unpredictable nature of the results in the past. The position of the jaw is key, not the plastic or specific device that holds it there. Another feature of a sleep device is that it should minimize impingement on the tongue. Sleep apnea and snoring is caused by the tongue and soft tissues falling back during sleep and obstructing the airway.
See attached link for a more comprehensive discussion: www.nhlbi.nih.gov/health/health-topics/topics/sleepapnea
We use the MicroO2 appliance at the PRP (physiologic rest position) of the jaw, determined by objective measurement, to treat these disorders.


MicrO2 Product Video
Nightlase Snoring Technique
An exciting adjunctive therapy for patient snoring and sleep apnea disorders is the use of our Lightwalker AT laser to help tighten the soft tissues at the back of the throat to improve the airway. See the attached link for more information on NightLase therapy: www.fotona.com/en/treatments/1627/nightlase/
Nightlase Procedure with Dr. Schiffmam
Interceptive Orthodontics
Years ago, we did full service orthodontic treatment. Today we only treat children between the ages of 4-9 (approximately) while they still have their primary teeth. Our goal is to encourage proper development of the jaws so that there is sufficient space for all their permanent teeth while the jaws and teeth are still growing. We want the jaw form of the child on the right; big broad arches and wide nasal passages. The child on the left has malformed arches due to a compromised diet and probably poor nasal breathing.
Critical to all of this is proper nasal breathing, which we discussed in a previous section, The Importance of Proper Breathing. There is lots of information on this topic connectingheads.com/articles/the-airway-breathing-and-orthodontics/
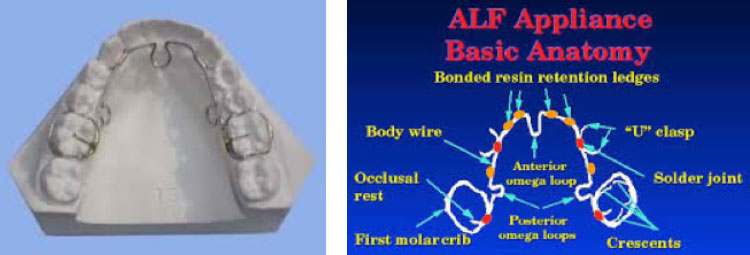
Much of our early treatment is with ALF appliances. We do not do braces and refer on to orthodontists to do the final fine tuning if required. www.alforthodontics.com/

Athletic Enhancement
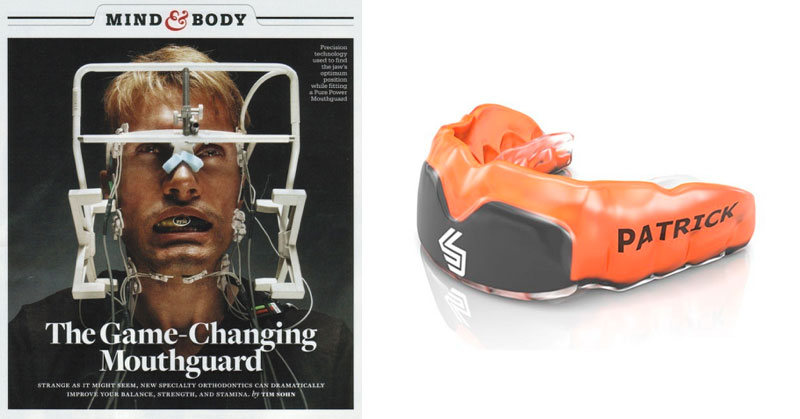
Specially designed oral appliances made to the PRP have made their way into professional athletics. A colleague of mine used the principles to develop the Pure Power Mouthguard which commercialized the product. However, it had only moderate success and minimal market penetration. Determining the correct PLP requires special measurement tools and a well-trained, experienced dentist. Again, it was not the plastic that was effective, but the jaw position. Micro-Dental labs out of California have picked up the ball and now can manufacture the PPM in an exclusive arrangement with Shock Doctor. The athletic appliances are made to the PLP tolerance determined by a trained dentist.
I have made many for elite athletes; the most significant success story being Tony O’Keefe. Here is a quote from his blog after completing RAAM (Race across America), a non-stop bicycle race from coast to coast.

“I went through the painless process of TENSing: relaxing and aligning the jaw, followed by a custom fitting by a specially trained dentist, Dr. Bob Clinton, … the results for me were instant. I returned to compete in RAAM in 2010 with my Elite PPM and surpassed expectations with a personal best performance, I felt strong and well balanced throughout the race’s 3000 miles and I credit my superior alignment and body posture to my PPM”
– Tony O’Keeffe (2010 RAAM competitor 10 days, 8 hours 21 minutes)
Since that time, the mouthguard technology has proved itself time and time again with many elite athletes.